1) 기본적인 grade
Hunt Hess Grade: a predictor of a patient's prognosis/outcome
|
Grade |
Characteristics |
Mortality Rate (%) |
|
0 |
Unruptured aneurysm without symptoms |
0 |
|
1 |
Asymptomatic or minimal headache and slight nuchal rigidity |
1 |
|
1a |
No acute meningeal or brain reaction but with fixed neurologic deficit |
1 |
|
2 |
Moderate to severe headache, nuchal rigidity, no neurologic deficit other than cranial nerve palsy |
5 |
|
3 |
Drowsy, confused, or mild focal deficit |
19 |
|
4 |
Stupor, moderate to severe hemiparesis, possible early decerebrate rigidity, and vegetative disturbance |
42 |
|
5 |
Deep coma, decerebrate rigidity, moribund |
77 |
Add on grade for serious systemic illness (severe atherosclerosis, HTN, DM, COPD, severe vasospasm on CTA)
WFNS grade
|
Grade |
Glasgow coma scale score |
Motor deficit |
|
I |
15 |
(-) |
|
II |
14-13 |
(-) |
|
III |
14-13 |
(+) |
|
IV |
12-7 |
(+) or (-) |
|
V |
6-3 |
(+) or (-) |
Aphasia, hemiparesis or hemiplegia
Fisher’s grade: Correlation between the amount of blood on CT & the risk of vasospasm
|
Grade |
CT findings |
|
1 |
No blood detected |
|
2 |
Diffuse thin layer of subarachnoid blood (vertical layers <1mm thick) |
|
3 |
Localized clot or thick layer of subarachnoid blood (vertical layers ≥1mm thick) |
|
4 |
Intracerebral or intraventricular blood with diffuse or no subarachnoid blood |
*measurements greatest longitudinal & transverse dimension on a printed EMI CT (no scaling to actual thickness) performed within 5 day of SAH
** “vertical layer” blood within “vertical” subarachnoid spaces including interhemispheric fissure, insular cistern, ambient cistern
Modified Fisher’s grade: Correlation between the amount of blood on CT & the risk of vasospasm

2) SAH 의심되는 환자 flow
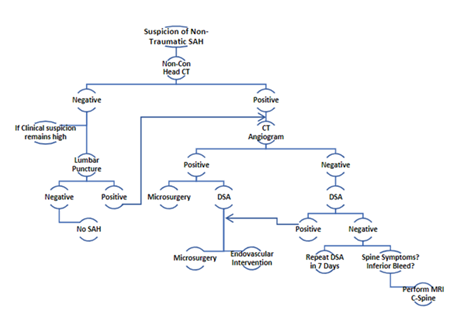
a. Initial Stabilization
1. Hydrocephalus: consider EVD
2. Blood pressure: SBP<160 with Nicardipine until the aneurysm is secured
3. Anti-fibrinolytic medication: when there will be a delay in treatment of the aneurysm. It does increase the risk of thromboembolic events.
4. Recommendation
A. Non-contrast CT (+) : CTA 시행, initial stabilization
B. Non-contrast CT (-) : 임상적으로 의심되는 경우 Lumbar puncture 고려
C. Lumbar Puncture: CT (-) 환자, RBC>1000 x 103/ml with xanthochromia
D. DSA: Initial (-) 인 경우, 1주 후 재시행하여 확진
E. MRI cervical spine: Initial DSA (-) 인 환자에서 cervical malformation을 R/O 하기 위해 시행 / Additional TL spine image if suspicious
b. Etiologies of SAH
1. Trauma (m/c)
2. Spontaneous
A. Ruptured intracranial aneurysm
B. AVM, Vasculitis, Tumor, Cerebral artery dissection ( may also be post-traumatic), Rupture of a small superficial artery, Dural sinus thrombosis, Spinal AVM, Cortical SAH, premesencephalic SAH
C. Coagulation disorders, Pituitary apoplexy
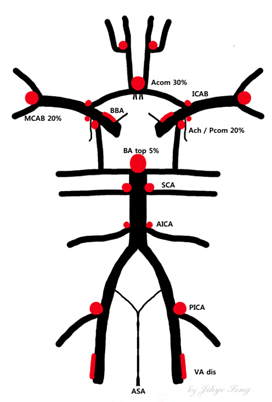
c. Aneurysm location
d. Treatment of SAH Sequelae
1) Vasospasm and delayed Neurologic injury
: 시기) ictus 3 – 14 days
A. Prophylaxis
1. Nimodipine for all patients with aneurysmal SAH 60mg q 4hr
2. Fluid status: euvolemic
3. Prevent hyponatremia: Cerebral salt wasting 으로 인한 Hyponatremia 주의!
4. Triple H
a. Hypertension (SBP 160-180, <200) ; norpin (norepinephrine)
b. Hypervolemia (CVP 8-12mmHg)
c. Hemodilution (Hct 30-32%)
d. Hypervolemia, hypertension; 예방적 사용은 additional complication..
B. Monitoring
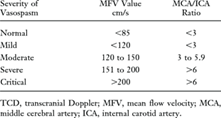
1. Transcranial Doppler; daily, 같은 혈관
2. CTA, CT perfusion: 본원에서는 현재 ictus 3일째 routine CT,7일째 도시바 CT 시행
a. CTP provides a quantitative measure of capillary level hemodynamics including MTT/CBV/CBF
b. to determine areas of hypoperfusion even in the setting of angiographically negative status / for early detection of tissue at risk
3. Consideration of EEG for patients with depressed exams
C. Work-up
: For any acute neurologic change, 다음을 의심하고 w/u 시행
rebleeding d/t same aneurysm or another hemorrhage source, hydrocephalus, infarct, cerebral edema, seizure, metabolic disturbance; hyponatremia.., hypoxia, sepsis
non contrast CT 시행하여 rebleeding 여부 확인 & lab check 하여 다른 원인 확인
CT (-) 인 경우, SBP <200으로 유지하며 윗년차/스탭 노티 하여 intervention 고려
증상 생긴 후 2시간 이내에 적극적으로 해야 효과 있다. 1시간 가량 적극적으로 혈압 올리고 수액 요법 하여도 효과 없으면 즉시 angioplasty 하도록 한다.
D. Treatment
1. EVT (angioplasty with IA vasodilator/balloon)
a. Papaverine; nonspecific smooth muscle relaxant which is no longer a mainstay of treatment d/t its side effect, esp. elevation of ICP
b. CCB: nimodipine/nicardipine/verapamil ; relax smooth muscle + direct neuroprotective effect by reducing free radical destruction of cells / last 12-24hr / S.E : systemic HoTN
2. HTN w/o hypervolemia
3. Maintenance of sodium levels
2) Hydrocephalus
3) Seizures
Low risk (1-7%), within <24hrs 에 발생
Prophylactic AED: not necessary unless the patient presents with seizure or undergoes clipping
Short course
Consider the use of EEG in patients with GCS <8
4) Other systemic effects
A. Cardiovascular system
Arrhythmia
|
SAH 후 나타나는 EKG상의 변화
* stunned myocardium: catecholamine and 칼슘이온의 과다노출로 인한 contraction band necrosis이며 reversible 하다. |
Neurocardiogenic injuries due to excessive catecholamine release
Monitor: ECG changes, vital sign abnormalities
Work up: cardiac enzymes, TTE ( for regional wall motion abnormalities)
Treatment: consider dobutamine, milrinone,
B. Pulmonary system
Pulmonary edema by catecholamine-induced decreased cardiac output
Pneumonia, aspiration pneumonitis, ARDS
Monitor: ventilator setting, Chest X-rays
C. Hematologic system
HIT- increased risk in SAH, due to heparin exposure during the intervention
Monitor: platelet count
w/u: HIT panel
Treatment: ensure not on heparin for DVT prophylaxis, consult Heme if counts continue to fall
D. Infections
Monitor: v/s, daily CBC
Medication
* nimodipine (nimotop)
Ca++ channel antagonist
For cerebral vasospasm prophylaxis
To improve outcome after SAH induced delayed ischemia
Adult: 60mg PG/NG q 4hr x 21 days
Nimodipine (iv)와 nimotop (oral)의 본원 사용은 iv 2주, oral 1주를 원칙으로 한다.
Iv 2주 이상과 oral 3T qid for 1주 이상은 보험 안되므로 절대 사용 불가
'신경외과 > Brain Anatomy (Basic, vessel)' 카테고리의 다른 글
| Occlusive cerebro-vascular disease (0) | 2020.11.24 |
|---|---|
| Intracerebral hemorrhage (0) | 2020.11.24 |
| Vascular malformations (0) | 2020.11.24 |
| Vascular anatomy (0) | 2020.10.09 |
| Basic anatomy (0) | 2020.10.09 |



